EVIDENCE OF ALTERED LUMBO-PELVIC MUSCLE RECRUITMENT IN THE PRESENCE OF SACROILIAC JOINT PAINSpine 2003. 28(14). pp1593-1600
1Barbara Hungerford PhD,2Wendy Gilleard PhD, 3Paul Hodges PhD
1School of Exercise and Sport Science, University of Sydney, Sydney, Australia
2School of Exercise Science and Sport Management, Southern Cross University, Lismore, Australia
3Department of Physiotherapy, The University of Queensland, Brisbane, Australia
Abstract:
Study design: Cross-sectional study of electromyographic (EMG) onsets of trunk and hip muscles in subjects with a clinical diagnosis of sacroiliac joint pain (SIJP) and matched controls
Objectives: To determine whether muscle activation of the supporting leg is different between controls and subjects with SIJP during hip flexion in standing.
Background: Activation of the trunk and gluteal muscles stabilise the pelvis for load transference, however the temporal pattern of muscle activation, and the effect of pelvic pain on temporal parameters has not been investigated.
Methods: Fourteen males with a clinical diagnosis of sacroiliac joint pain and healthy age-matched controls were studied. Surface EMG activity was recorded from seven trunk and hip muscles of the supporting leg during hip flexion in standing. Onset of muscle activity relative to initiation of the task was compared between groups, and between limbs.
Results: Onset of obliquus internus abdominis (OI) and multifidus occurred prior to initiation of weight transfer in the controls. The onset of OI, multifidus, and gluteus maximus was delayed on the symptomatic side in SIJP subjects compared to controls, and the onset of biceps femoris EMG was earlier. In addition, EMG onsets were different between the symptomatic and asymptomatic side in subjects with SIJP.
Conclusions: The delayed onset of OI, multifidus, and gluteus maximus EMG of the supporting leg during hip flexion, in subjects with SIJP, suggests an alteration in the strategy for lumbo-pelvic stabilisation that may disrupt load transference through the pelvis.
Key Words:
Sacroiliac joint, pelvic stabilisation, motor control, electromyography, low back pain, pelvic pain
Key Points
- Activation of obliquus internus abdominis (OI) and lumbar multifidus occurred prior to onset of motion in control subjects.
- Subjects with a clinical diagnosis of sacroiliac joint pain show delayed onset of EMG activity of OI, multifidus, and gluteus maximus compared to control subjects.
- The delay in onset of OI and multifidus EMG as subjects stood onto one leg occurred on both the symptomatic and asymptomatic side in the group with sacroiliac joint pain. In comparison, bicep femoris activation occurred earlier in the group with sacroiliac joint pain.
- The delayed onset of OI, multifidus, and gluteus maximus EMG on the supporting leg during hip flexion, in subjects with sacroiliac joint pain, suggests an alteration in the strategy for lumbo-pelvic stabilisation that may disrupt load transference through the pelvis.
Acknowledgments
The authors wish to acknowledge Ray Patton and Dr Roger Adams, from the Faculty of Health Sciences, University of Sydney, respectively for technical and statistical advice. Financial support for PH was provided by the NHMRC of Australia.
Discussion (excerpt)
This study has shown for the first time that subjects with a clinical diagnosis of SIJP show delayed onset of EMG activity of OI, multifidus, and gluteus maximus compared to control subjects. The delay in onset of OI and multifidus EMG as subjects stood onto one leg occurred on both the symptomatic and asymptomatic side in the SIJP group. In comparison, bicep femoris activation occurred earlier in subjects with SIJP.
The present results indicate that onset of EMG of OI and multifidus occurred prior to initiation of motion in control subjects. This is consistent with previous research that has identified feedforward activation of TrA, OI and multifidus in association with limb movements that challenge the stability of the spine9,10,36. Previous studies have suggested that TrA and OI, in particular the lower fibers that are orientated horizontally, may contribute to compression of the SIJ1. Similarly, lumbar multifidus activation may increase tension on posterior SI ligaments and posterior layer of the thoraco-lumbar fascia3, and induce a nutation force on the sacrum37. Pre-activation of OI and multifidus, as determined in this study, may therefore contribute to compression of the SIJ prior to initiation of single leg stance, in order to produce optimal pelvic stabilisation for load transference. Pelvic stability may have been further enhanced by the combined activity of OI and adductor longus, producing compression of the pubic symphysis5. In contrast, biceps femoris EMG was decreased at initiation of motion in control subjects. This reflects findings of previous research in which little activity of biceps femoris was identified when standing on one foot38.
In the SIJP group the onset of OI, multifidus, gluteus maximus, and bicep femoris EMG was significantly different on the symptomatic side compared to the asymptomatic side, and control subjects. OI and multifidus activation occurred more than 80ms after initiation of motion and cannot be considered to be feedforward. This would suggest a change in the motor control strategy on the symptomatic side in subjects with SIJP. Similar results have been found in subjects with pain in the lumbar origin8,17. …….
Identification of an altered pattern of muscle recruitment in subjects with SIJP is significant for the conservative management of lumbo-pelvic pain. Previous research has shown specific exercise treatments are effective in altering pain and functional disability in patients with segmental lumbar instability and altered motor recruitment patterns41,42. Further research is required to determine if the altered pattern of muscle recruitment identified in subjects with SIJP may be similarly improved with specific exercise intervention.
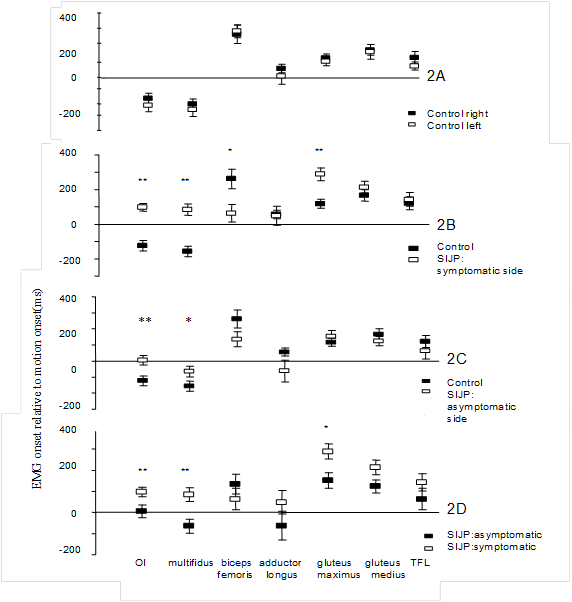 |
Figure 2. Mean time of EMG onset for the supporting leg during hip flexion in standing in 2A: control subjects; 2B: control subjects versus SIJP subjects on the symptomatic side; 2C: control subjects versus SIJP subjects on the asymptomatic side; 2D: asymptomatic versus symptomatic side in SIJP subjects. Standard errors of the mean are shown. *p £ 0.05; **p £ 0.01. Note the significant delay in OI, multifidus, and gluteus maximus activity on the symptomatic side in SIJP subjects in comparison to control subjects, and the asymptomatic side. |